Introduction
The EU security and defence landscape has changed over time from the European Security Defence policy (ESDP) to the Common Security and Defence policy (CSDP). Changes regarding CSDP derive from the different types of documents. The most important are legal acts and strategic policy documents (such as Treaty of Lisbon and Global Strategy). Changes are based on the EU’s external and internal situation. The latest and most important influencing force for the EU and the whole world is the COVID-19 pandemic, which has caused changes not only in the legal acts and policy planning documents, but also in human minds. The unexpected global challenge has meant issues regarding the ability of the countries to overcome pandemics and the possibility of strengthening prestige.
In the EU, the pandemic has shown for the need for a coordinated and comprehensive strategy to deal with health emergency needs, to support economic activity, to prepare the ground for the recovery, and to be prepared for future challenges. The CSDP has a variety of instruments – tools designed not only to improve, strengthen and develop the field of defence, but also to strengthen civil-military cooperation and to build confidence in each EU member states’ policies. CSDP has different tools, the most visible are EU military missions and operations, but Permanent Structured Cooperation (PESCO) is one of the most important CSDP instruments. Until 2017, it was an unknown tool in practice, incorporated in the Treaty of Lisbon, but now 47 projects within PESCO are implemented. Two of the PESCO projects deal with medicine.
The COVID-19 crisis has shown that states should use many tools to overcome a pandemic and promote prestige. Therefore, the aim of the study is to identify whether PESCO can be one of the tools for future projects in medicine, whether it can help in future pandemics, whether it can also be used to strengthen the military medicine of the EU and, simultaneously, be in synergy with the civilian sector by providing support to the civilian field, and whether EU member states can increase their prestige through PESCO.
The empirical part of the study is based on Latvia’s case, but the theoretical framework is built on prestige in the view of the school of realists of international relations. The study is based on qualitative research methods.
Basic aspects of prestige
Prestige, rather than power, is the modern-day currency of international relations (Gilpin, 1981, p. 31). Prestige is an extremely important tool because as soon as an actor’s strength is acknowledged, his or her goals cannot be achieved by using it. The definition of prestige has weaved through history, directly and indirectly affecting social sciences, yet the academic focus that the concept has attracted, with its ability to influence politics, has been irregular.
When looking towards the development of the definition of international prestige in the sphere of international relations, its roots can be found within realist school theories, as the definition of prestige in international relations developed alongside the development of classical realism. A State’s internal and international policies, in the view of Morgenthau (1984, p. 21), are two manifestations of the same phenomenon – the struggle for power.
However, analysis of both domestic policy and international relations reveals three main policy types – policies to maintain power (status quo policies), strategies to expand power, and systems to demonstrate it. The definition of prestige is related to and explains the third international relations policy type – demonstrating power. Even though realism is characterised by the central role of power in international relations, Morgenthau does not consider prestige to be an end in itself for a State’s foreign policy. In his interpretation, Morgenthau (1948, p. 50) differentiates prestige policies from those of maintaining power or expanding it. In his view, prestige policies are an instrument with which status quo or imperialist policies attempt to achieve their goals. Due to this, prestige in national relations is a fundamentally inherent element, and the desire for prestige in international relations is comparable to the same passion for it between individuals.
Morgenthau (1948, p. 51) evaluates that the place of prestige in the anarchy of international relations is inherent because only through a State’s reputation can it achieve the goals of international relations - power, peace, and welfare. In the fight for existence and power, what others think about us is just as important as what we truly are. Prestige is a player’s reflection in the eyes of the international community, and this reflection, rather than the original, determines what role we, as members of society, play. For this reason, the task of prestige is to ensure that the international community’s mental picture of the actor would resemble the one which the State sees itself as or an even better version of it.
The two central prestige policies that ensure this goal are 1) diplomatic ceremonies and 2) the demonstration of military power. The function of prestige policies stems from the nature of international relations. Namely, the actors’ foreign policy is formed by the current assessment of global power relationships and their expected development. The function of prestige policies is to utilise these international power relationship assessments in ways that benefit the actor (Morgenthau, 1948, p. 56). In Morgenthau’s (1948, pp. 58–60) assessment, the most massive prestige policy errors are exaggerated bluffing, and negligent behaviour against prestige and the reputation of the country as a whole, relying solely on the player’s known objective realities – military power.
Prestige is the reputation of power, especially military power. While power concerns actors’ economic, military, and other related capabilities, prestige relates to another state’s perception as regards the player’s abilities and its desire to implement them. Prestige is about perception and the credibility of an actors’ power. Therefore, power is different from the perception of power (Gilpin, 1981, p. 31). Most authors do not differentiate these terms in their analysis, even though prestige and reputation, while closely related, are different terms. Following Robert E. McGinn’s (1972, pp. 103–105) approach, reputation unifies the community’s opinion about a specific player, while prestige is an indicator of favourable views that encompasses ‘grace’ and approval. Both prestige and power, in a broad way, include quantitative indicators, while prestige, as opposed to power, also possesses qualitative indicators – the positive opinion of other players. Therefore, an essential component of prestige is respect and favourable intentions, while for reputation, these components are not necessary. Prestige is a respectful attitude and benevolence about the player’s achievements in a particular field (McGinn, 1972, pp. 103–105).
Overall, in the context of the tradition of realism, prestige plays a downstream role, i.e., it acts as an aspect of preservation or expansion of power. Prestige provides opportunities for the development of power and, at the same time, deterrence of aggression.
Prestige is a State’s or a group of States’ perceptions about a different actor or a group of actors’ excellence. This excellence recognised by other players furthers the respective player’s growth in power. Even though prestige is an element of international relations, prestige policies are not independent or self-targeting. Prestige policies are the player’s tool for the maintenance of power, expansion of power, and deterrence of aggression. In this analysis, an essential instrument of prestige is financial or political aid, including projects of interest to the international community or the region. Even though political and financial assistance are not critical elements for the existence of prestige, they nevertheless contribute to its sustainability.
Prestige, for small prestige-seeking actors such as Latvia, plays a vital role. Being a part of international organisations and projects implemented by them is very important and often the only instrument that a small country has to promote its prestige and cooperation vectors on the international stage.
The case of Latvia is chosen as a case study of prestige promotion. Latvia’s contributions to international organisations work not only as foreign policy goals in the framework of security concerns, but also as a hope of increasing their standing and prestige amongst NATO and European allies. Considering the number of small states across the globe, the value that their collective impact has on international organisations is crucial. Thereby, by promoting their prestige, small prestige-seeking states also provide significant benefits to their member organisations and programmes they implement in the long term, such as PESCO.
Also, in the COVID-19 crisis, PESCO can be an opportunity and an important instrument to promote countries’ prestige and, simultaneously, be a way to overcome a pandemic. Further on in the paper, the authors will explore the PESCO legal framework, analyse PESCO development and PESCO projects in medicine, apply Latvia’s case, and identify potential medical field directions.
PESCO legal framework
With the coming into force of the Lisbon Treaty in 2009, EU countries initiated significant changes in the field of EU defence – the most important was the launch of CSDP. With the Lisbon Treaty, EU countries amended regulations regarding security and defence in the Treaty on European Union (the Maastricht Treaty). CSDP is the main element of the EU’s Common Foreign and Security Policy, it has different tools in the fields of defence and crisis management; some of them are widely used, but some have not been used since their creation (for example: the collective self-defence clause, EU military missions and operations, EU Battle groups, PESCO). Decisions on CSDP should be taken by the Council by unanimity. However, decisions relating to PESCO require a qualified majority. Additionally, it is necessary to point that the pandemic crisis in Europe calls for the application of subsidiarity (Article 5) and solidarity principles (Article 24) from the Treaty on European Union and think about other tools from the legal framework to overcome crisis. For instance, in the Treaty on the Functioning of the European Union, Article 222 contains a solidarity clause. It is lex specialis, mentioned outside the CSDP frame, and it can serve as an umbrella to overcome threats other than military under mutual cooperation. This is analysed separately.
With regard to PESCO, it is worth mentioning that it is the most unusual of CSDP tools and was not implemented until 2017. PESCO was included in the European Constitution, which was not ratified. Later, it appeared in the Lisbon Treaty. The importance of all CSDP tools, especially PESCO, in the long term, should be related to Article 42(2) of the Treaty on European Union, which states that CSDP includes the progressive framing of EU defence policy and it can lead to a common defence. In such a case, the European Council should make a decision unanimously.
The Lisbon Treaty amended the Treaty on European Union, and the Treaty on the Functioning of the European Union. The basis of PESCO derives from the Treaty on European Union Article 42(6), 46, and the additional protocol 10. PESCO is one of the mechanisms for implementing the principle of differentiated integration or flexibility. In fact, PESCO has no direct predecessor in EU law; it is a rare genuine novelty. PESCO is different from other forms of cooperation because it is legally binding framework for deeper cooperation. It means that participating EU member states have legal obligations which derive from the Council decision for establishing PESCO and EU law. Biscop (2018, p. 163) explains that PESCO projects mean collective engagement; therefore, it is difficult to withdraw from them.
Article 42(6) is a general clause of PESCO, stating that EU Member States with military capacity that fulfil higher criteria and have common commitment in this area can establish PESCO (Consolidated version of the Treaty on European Union, 2012, p. 2). Naumescu (2018, p. 67) points out that political commitment means that PESCO is strategy and policy at the same time. Additionally, to Article 42(6), it is essential to take into account Article 46, which is divided into six interrelated parts – the most important are the first five. The first part determines that EU member states must inform the Council and the High Representative of the Union for Foreign Affairs and Security Policy of their intention to establish PESCO; The second part includes three months for the Council to decide on PESCO; in accordance with the third part, any State must inform both the Council and the High Representative of its intention to join PESCO; the fourth paragraph sets out the criteria and authority for the Council to decide to suspend a member state’s participation in PESCO; the fifth part allows PESCO states to withdraw from PESCO projects by informing the Council (Consolidated version of the Treaty on European Union, 2012, p. 2).
Additional protocol 10 consists of a preamble and three articles. According to the contract, membership in PESCO is open to any EU member state (Article 1), which undertakes to develop its national defence capabilities faster, and further in the protocol, the possibility of being involved in the European Defence Agency, the main European equipment programmes, and multinational forces are not excluded (Treaty on European Union, 2012, annex 10). PESCO states should have the capacity to supply multinational force groups, targeted combat units (including transport and logistics, etc.) to carry out tasks within a period of 5 to 30 days, and which can be continuous for an initial period of 30 days and be extended up to at least 120 days (Treaty on European Union 2012, annex 10). In the protocol, Article 2 contains five paragraphs containing obligations: cooperation, harmonisation of military needs, measures to enhance the availability, interoperability, flexibility, and deployability of forces, working together and involved in European equipment programmes (Treaty on European Union, 2012, annex 10). Based on the legal framework, the issues regarding PESCO have changed significantly since 2017, influencing not only each EU member state but an understanding of EU capabilities in the world as well. For CSDP development, PESCO is one of the greatest leaps since EU Global Strategy came into force in 2016. Importantly, the objective of PESCO is to achieve the full spectrum of defence capabilities available to missions and operations, increase the EU’s military capacity internationally, promote protection of EU citizens and foster the effectiveness of defence spending. It raises a question about the development cycle of PESCO and the areas of PESCO projects?
PESCO development and projects in field of medicine
Discussions regarding PESCO occurred before the Lisbon Treaty was signed, but after the Lisbon Treaty came into the force, and until 2017, PESCO was only on paper as a tool, but never implemented and used for EU needs. It is essential to point out that during the Italian presidency in 2003, the whole mechanism was modified from “structured cooperations” to “permanent structured cooperations” (Blanke and Mangiameli, 2013, p. 1281). 2017 was a turning point, and PESCO’s full potential is still unknown (the PESCO development cycle/timeline appears in Table 1). The most important trigger points for CSDP and PESCO were the Russian aggression in Ukraine, Brexit, and the election of Trump. PESCO is an essential tool, but what can PESCO provide for the field of medicine and countries’ prestige?
Table 1
PESCO development time-line (PESCO secretariat a, no date)
Four necessary steps were made regarding PESCO in 2017 – the Council agreed on the necessity of PESCO, 23 member states signed a notification on PESCO, two additional countries joined the signed notification and, as a result, the Council formally established PESCO (PESCO secretariat a, no data). The participation of third countries (Norway, post-Brexit United Kingdom (UK), etc.) in PESCO projects is still topical. Leuprecht and Hamilton (2019, p. 80) conclude that the model for third countries’ involvement in PESCO is provided by the European Defence Agency, but it needs to be improved. The UK is a military power and its withdrawal from the EU changed existing EU strategy and influenced all EU Member states’ defence and security strategies. According to Sweeney and Winn (2020, p. 242), Brexit decreases UK influence on EU defence and security policymaking and its impact on the EU CSDP instruments. Nevertheless, PESCO is a route back for the UK.
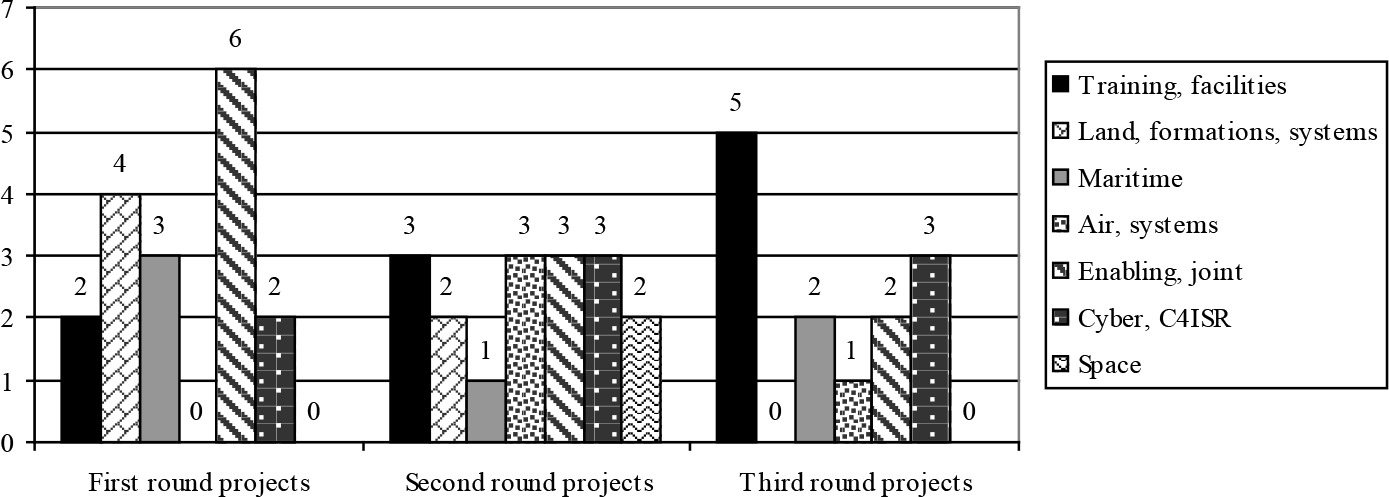
The Council’s formal decision, the “Schengen Defence” or “the Eurozone of Defence”, was finally created. Legal conclusion and binding commitment was the basis for future projects within PESCO. In three stages, the EU started to carry out 47 PESCO projects: on 6 March 2018, the Council adopted the first 17 PESCO projects, the second list of 17 projects under PESCO was approved by the Council on 19 November 2018, but on 12 November 2019, the Council adopted the third list of 13 PESCO projects. All the PESCO projects Dossi (2019, p. 3) concluded that Germany and France are the “core states” of the projects. All PESCO projects are grouped according to the covering areas (Figure 1).
From all 47 PESCO projects, only two are related to the field of medicine: the European Medical Command and Special Operations Forces Medical Training Centre (SMTC) – they make up only approximately 4% of all the projects. The European Medical Command project was among the first approved projects, but the Special Operations Forces Medical Training Centre was included in the third approved list of PESCO projects (European Defence Agency, 2020). The coordinator state in the European Medical Command project is Germany and there are 11 EU member states in this project, but in the Special Operations Forces Medical Training Centre, the leading state is Poland and Poland is the only EU member state involved.
European Medical Command is a specific formation because its headquarters are in Brussels, and the main idea is that it ensures that the EU has medical capabilities and coordinates medical resources (PESCO secretariat b, no date). One of its obligations is to be responsible for joint limited EU medical services (planning, management, coordination, etc.) and to create a multinational specific medical unit with the option to deploy it for basic primary care and evacuation of people/soldiers from the operational area (Nielsen, 2017). The idea of the European Medical Command project is to provide a common medical picture according to the operational situation and assist in the harmonisation of medical standards, legal framework, and principles of sanitary service (PESCO secretariat b, no date). It is one of those projects the EU needs to become a more credible military power. All projects related to military Special Forces are distinct and specific – the same can be said about the Operations Forces Medical Training Centre, because its primary purpose is medical training and being an excellent centre in the field of special operations. It is necessary to increase medical support for special services. There are two projects established for medical cooperation, but they do not function in practice. After some time, the results will probably be visible from both projects as can be said about other PESCO projects as well.
From the perspective of EU capacity, development in the field of defence is positive because, among all PESCO projects, two have a medical direction, but at the same time, it is strange that these projects cover only 4% of all PESCO projects. EU Member States are not active and interested in this field but, in time, when the whole world is affected by COVID-19, it is a challenge and necessity to establish new projects in the field of medicine and such projects should have close civil-military cooperation. In times of crisis, by proposing or negotiating such projects, countries would increase their visibility, position of power, and enhance their prestige. Almost all EU Member States are involved in PESCO and lot of them are small states and they do not have real power internationally, but with nonstandard behaviour, they can acquire better positions. Thereby, EU Member States would not only promote prestige, but it would be a unique tool not only in the military but in the civilian sector as well, because all military projects can be used in the civilian sector. The projects can be implemented in the form of direct support to combat Covid-19 or indirect support through technology to medical personnel, especially at a time when medical staff are involved in the fight against the pandemic. Military aid can provide specific support to everyone, not just soldiers on the battlefield. It is especially important for small states. For those who are not familiar with military medicine, it raises lot of questions and, therefore, when analysing Latvia’s case, writers will mention levels of military medicine, explore how to become a specialist in military medicine, how the support provided by military medicine is distributed, and at what level the civil-military synergy in medicine Is.
Aspects of military medicine and the Latvia’s case
The military field and military policy are specific for each EU country, and medical issues have an essential aspect. In the field of military medicine, medical support is divided into different levels, necessary because medical support for soldiers must be provided in different conditions, including on the battlefield. In this article, as an example of military medicine level classification, the authors will apply the 2019 NATO Standard publication AJP-4.10 “Allied Joint Doctrine for Medical Support.” In the publication, military medicine is divided into four levels (Role 1; 2; 3 and 4). Classification is based on each task’s specifics, the size of the involved forces, the required assistance level, and speed, the risk and challenges that soldiers and medics may face and so on. Medical staff must be able to adapt to a wide range of conditions and, at the same time, provide appropriate medical care – from lower to higher: Role 1 (R1) is a set of primary health care, it includes triage, first aid, pre-hospital care, primary and essential diagnostic, limited medical care, patient holding and medical supply capacity; Role 2 (R2) is a set of abilities to increase surveillance by supplementing the Role 1 level, it includes stabilising the patient’s condition for transportation to the medical institution, which provides daily medical care, life-saving surgery, laboratory examinations, dental care and radiological diagnostics; Role 3 (R3) consists of a set of deployable specialists, a set of hospital care capabilities – these capabilities should include computer tomography (CT) and oxygen and with these tools, higher level of care before evacuation can be achieved (in fact it is either a military hospital or civilian hospital in a safe zone with military or civilian medics); Role 4 level (R4) includes the full spectrum of medical care (e.g. specific attention: reconstructive-surgery, prosthetics and rehabilitation), at the level of national responsibility and, therefore, it is provided by civilian medics in civilian medicine institutions (Allied Joint Doctrine For Medical Support, 2019, s. 2). In the case of Latvia, military medical centres are located at military bases. If necessary, these centres can provide support not only to soldiers, but also to the civilian sector.
For a broader understanding, it is necessary to mention a regulation about the field of military medicine in Latvia from national legal acts. In Medical Treatment Law, it is embedded in a definition of military paramedics and requirements for military medical professions (Article 45.4 and 45.5) – it has a basis in Latvia’s legal acts for a paramedic. However, an additional and more detailed regulation is included in the regulations of the Cabinet of Ministers (Medical Treatment Law, 1997, c. VII C.). Consequently, according to the regulation, the competence of a paramedic includes (Noteikumi par ārstniecības, 2009, c. 7.17): health examination, primary evaluation after injuries, medical triage (victim sorting), establishing the fact of death during operations, and theoretical and practical skills covering a wide range of issues (emergency medical care, injury care, environmental disorders, acute infections, etc.) (Noteikumi par ārstniecības, 2009, c. 7.17). The Cabinet of Ministers has also approved the medical institutions’ requirement in the Latvian National Armed Forces (NAF). According to the regulations, (Noteikumi par ārstniecības, 2009, c. 6.1) the medical institutions of NAF should provide primary and secondary health care and outpatient health care to the NAF soldiers and the National Guard, and ensure a day hospital. These types of institutions must meet the general requirements which are set for all medical institutions. They should have administrative and utility rooms, medicine storage rooms etc. (Noteikumi par ārstniecības, 2009, c. 6.1). Information about civilian and military institutions and their location is available in the register of medical institutions (Medical Inspection, 2020). The most important regulation at the Cabinet of Ministers level regards extended first aid. This type of medical care can be provided to soldiers and representatives from the National Guard as well. According to the regulation (Noteikumi par ārstniecības, 2009, article 2), extended medical attention should be offered to soldiers and National Guard representatives who are in a critical condition and this type of care includes care with appropriate medical equipment etc. (Noteikumi par karavīru, 2010. c. 1 and annex 4). To provide extended first aid, both representatives from the National Guard and soldiers have to complete a unique training programme (in cases when such a programme is finished abroad, it can be matched). Each soldier must have an individual medical kit, but the rescued soldier has a specific package – this type of equipment is much bigger and should include 42 items according to the regulation (Noteikumi par karavīru, 2010. c. 1 and annex 4). To provide the most effective assistance and to save lives, civilian and military medics need a variety of technological innovations. It is vital to have civil-military synergy because it is much cheaper, and there is one common goal from the perspective of state policy, but what are the best directions for projects if they are implemented within PESCO? Latvia and other countries, by proposing projects for discussions under PESCO in the field of medicine (including an epidemic), would promote its recognition and prestige politically and strengthen military capacity by implementing projects. COVID-19 has shown that such projects can foster and enhance cooperation and trust between EU member states and increase their prestige. What are the potential directions and benefits?
Potential directions in the field of medicine and benefits
Any question can be initiated at the level of policy discussion, but directions for the first steps can be different and in the field of medicine too. COVID-19 has shown that medical care can be linked to crisis conditions, it is a challenge – as on the battlefield, because the number of victims increases all the time and the assistance provided varies. In such situations, equipment, facilities, and capabilities are limited. On the battlefield, individual medical kits and soldiers’ rescue medical kits are notably available for soldiers, but specific medical devices and treatment are only provided in hospitals.
With regard to the field of medicine, including civil-military synergy, different types of projects can be initiated and implemented under PESCO, e.g. a new kind of transport for evacuation - medevac (a particular vehicle for military or civil needs, which can be armoured and with specialist equipment etc.), a new type of medical device which can be used on a tactical level and in civil hospitals, creation of new regional laboratories and research centres, modern analytical and biotechnological equipment development, improvement of logistic chains (easier delivery and documentation etc.), the establishment of unique and specific training institutions for civilian and military medics (including the development of specific 3D education programmes etc.), and the use and development of robotic technologies or drones.
These directions are an example that can serve as a basis for discussions, for specific projects that are useful both at the national and regional levels, thus strengthening the EU’s overall capabilities and the prestige of certain countries. For COVID-19 and potential directions for projects, an expert in the field of military medicine explained that: firstly, they should be models for action in the field of public health safety in the form of already approved procedures and algorithms for different epidemiological situations, leading to cross-border cooperation between EU bodies for redistribution and supply, to provide up-to-date, validated epidemiological information quickly and centrally; secondly, the direction should be to consolidate the scientific resources of the EU countries for the necessary joint research, such as the development of a vaccine; thirdly, the EU’s civil protection rapid response capability should be developed by increasing its preparedness and integrating it with NATO procedures and skills (Anon, 2020).
The medical field is one of the most important and evidence for that is COVID-19. Countries that engage in epidemiological security measures during COVID-19 are clearly enhancing their prestige by not only demonstrating their readiness to react to the current situation, but also by taking practical action. PESCO can be one of the tools to promote prestige of individual EU Member States – especially small states. That is not only aimed at achieving a proactive and effective goal in a corporate environment but is also able to establish a basis for further common procedures and procedural actions, which is essential for planning the activities of other similar crises. It is not a one-size-fits-all act but a constant development, creating a systematic self-sufficient structure for emergencies (Anon, 2020). Developed medicine projects for military needs can be used for the civilian sector as well. This would be a way to increase civil-military synergy and improve states’ prestige. By analogy with NATO, the EU should develop the applicability of common medical technologies, including the processing and circulation of electronic medical data, telemedicine, and the synchronisation of the competencies of interoperable medical specialties should be continued – it would be essential to create a unified health care management system (Anon, 2020). These directions would allow the effective organisation of health care activities to be systematised to achieve the goal.
It means EU countries can save resources because they can achieve specific and different projects together. EU countries, to identify best directions for developing projects in the field of medicine, should involve EU military medicine companies in this process. Latvia’s involvement in various courses in medical areas within PESCO would allow strengthening of not only the military but also the civilian medicine sector. For Latvia, the field of medicine is, importantly, well developed with an extensive network of medical institutions and personnel, and a good potential for research provided by education institutions (for example, Riga Stradiņš University etc.), where world-famous pharma companies are located (for example, Gridex, Arbor Medical Company.). Besides this, it is essential to point out that the issues related to military medicine are specific because they have protection under International Humanitarian Law; therefore, it is an advantage for developing projects in this direction. The Additional Protocol of Geneva Conventions states that medical personnel must be respected and protected. It must ensure that medical units during warfare, such as transport and staff, are identifiable and that medical personnel, buildings, and units are distinguished (protection is based on the distinctive emblems – the Red Cross, crescent, lion and sun form) (Protocol Additional to the Geneva Conventions, 1977).
It should be noted that in cases when the aggressor state violates special medical regulations, the other party may internationally draw the attention of other states to the violations, thereby discrediting the aggressor. If countries follow the rule regarding the protection of medical personnel and institutions, this area is potentially less affected during warfare and results in less damage and loses. Only time will show whether we have benefited from the COVID-19 crisis and used all the opportunities available. PESCO can serve as a way to promote prestige and to gain other benefits for the civilian and military sector.
Conclusions
Prestige is not an end in itself for national foreign policy. The prestigious system is one of the tools by which an actor can achieve its goals within the status quo environment. Prestige, rather than power, is the modern-day currency of international relations. Prestige can also be identified as a reputation of power, especially the military. It is about perception and the credibility of an actors’ ability, which provides opportunities for the development of power and, at the same time, deterrence of aggression. PESCO could work as one of the tools for the projects within the EU in the medical field and can also provide an opportunity for countries to promote their status on the international stage.
With the coming into the force of the Lisbon Treaty in 2009, EU countries initiated significant changes in the field of EU defence, the most important was that CSDP was launched. From all CSDP offered tools, PESCO is the most unusual, and it was not implemented until 2017. The legal framework of PESCO is included in the Treaty on European Union Article 42(6), 46, and additional protocol 10. PESCO is one of the mechanisms for implementing the principle of differentiated integration or flexibility. The basic idea of PESCO is to achieve the full spectrum of defence capabilities for EU missions and operations, increase the EU’s military capacity, take care of EU citizens and promote the effectiveness of defence spending. The pandemic crisis in Europe calls upon the application of subsidiarity (Article 5) and solidarity principles (Article 24) from the Treaty on European Union and identifies and applies other tools from the EU legal framework to overcome the pandemic.
In 2017, four necessary steps were made – the Council agreed on the necessity of PESCO, 23 member states signed a notification on PESCO, two additional countries joined signed the notification and, as a result, the Council formally established PESCO. In three stages, the EU started to carry out 47 PESCO projects: on 6 March 2018, the Council adopted the first 17 PESCO projects, the second list of 17 projects under PESCO was approved by the Council on 19 November 2018, and on 12 November 2019, the Council adopted the third list of 13 PESCO projects.
Of all 47 PESCO projects, only two are related to the field of medicine: European Medical Command and Special Operations Forces Medical Training Centre (SMTC) – approximately only 4% of all projects. One of the tools within CSDP to strengthen the field of medicine, especially at a time when the whole world is affected by COVID-19, is PESCO. It is a challenge to establish new projects in the field of medicine and such projects should have close civil-military cooperation. It would be a unique tool not only in the military, but in the civilian sector as well. It can be implemented in the form of direct support to combat Covid-19 or indirect support through technology to medical personnel, especially at a time when medical staff are involved in the fight against the pandemic. In the field of military medicine, medical support is divided into different levels (Role 1; 2; 3 and 4). In Latvia’s case, a regulation about the field of military medicine comes from national legal acts – Medical Treatment Law and several Cabinet of Minister’s regulations. PESCO can be one of the tools to promote the prestige of individual EU Member States – especially small states such as Latvia. To provide the most effective assistance and to save lives, civilian and military medics need a variety of technological innovations. It is vital to have civil-military synergy because it is much cheaper, and there is one common goal from the perspective of state policy. COVID-19 has shown that projects in medicine can foster and enhance cooperation and trust between EU member states and increase their prestige. In the COVID-19 situation, medical care can be linked to crisis conditions; it is a challenge, as on the battlefield, because the number of victims increases all the time and provided assistance varies. In such situations, equipment, facilities, and capabilities are limited.
In the field of medicine, including civil-military synergy, different types of projects can be initiated and implemented, for example, the new kind of transport for evacuation - medevac (a particular vehicle for military or civil needs, it can be armoured and with specialist equipment etc.). A new type of medical device can be used on a tactical level and in civil hospitals, creating new regional laboratories and research centres, modern analytical and biotechnological equipment development, improvement of logistic chains (more natural delivery and documentation, etc), the establishment of new and specific training institutions for civilian and military medics (including the development of specific 3D education programmes etc.), and the use and development of robotic technologies or drones.
These kinds of projects should first be models for action in public health safety in the form of already approved procedures and algorithms for different epidemiological situations:
It would help cross-border cooperation between EU bodies’ redistribution and supply, and provide up-to-date, validated epidemiological information quickly and centrally.
It should be possible to consolidate the scientific resources of EU countries for necessary joint research, such as developing a vaccine.
The EU’s civil protection rapid response capability should be formed by increasing its preparedness and integrating it with NATO procedures and capabilities.
Countries that engage in epidemiological security measures during the COVID 19 pandemic are enhancing their prestige by demonstrating their readiness to react reactively and taking practical actions. That is not only aimed at achieving a proactive and effective goal in a collaborative environment, but also establishing a basis for further common procedures and procedural actions, which is essential for planning activities in other similar crises. It is not a one-size-fits-all act, but a constant development creating a systematic self-sufficient structure for crises.
By analogy with NATO, the EU should develop the applicability of common medical technologies, including the processing and circulation of electronic medical data, telemedicine, and the synchronisation of the competencies of interoperable medical specialties should be continued – it would be essential to create a unified health care management system. This means EU countries can save resources because they can carry out specific and different projects together. EU countries, to identify best directions for developing projects in the field of medicine, should involve EU military medicine companies in this process.
Latvia’s involvement in various directions in medical fields within PESCO would allow the strengthening of not only the military, but also the civilian medicine sector. For Latvia, it is important that the field of medicine is well developed with an extensive network of medical institutions and personnel, good potential for research, provided by education institutions where various pharma companies are located.
The thematic field changes over time for activities in the field of medicine and defence. Changes require wider discussion and different thinking, which can lead to the implementation of sustainable and high-quality projects, increasing the efficiency and flexibility of using resources. Issues related to military medicine are specific because they are protected under International Humanitarian Law. Therefore, it is advantageous to develop projects in this direction, and PESCO is a tool for new projects in medicine.
Although the COVID-19 crisis has been a significant challenge for the world as a whole, it has also taught us a lot and provided material for the development of new research, both academically and practically. The areas analysed in this article are extremely topical and will not lose their relevance in the nearest future. It serves as a strong basis for further study, which altogether can serve as a complementary element for more comprehensive policies within the existing initiatives.